
Hiatus Hernia and Gastroesophageal Reflux Disease (GERD)
Hiatus hernia and gastroesophageal reflux disease (GERD) are common gastrointestinal conditions that can significantly impact a patient’s quality of life. Hiatus hernia occurs when a portion of the stomach pushes through an opening in the diaphragm into the chest cavity, while GERD is characterized by the backward flow of stomach acid into the esophagus, leading to reflux symptoms. Hiatus hernia, also known as a hiatal hernia, can contribute to gastric reflux. When symptoms persist despite treatment, laparoscopic surgery may help provide long-term relief.
Hiatus Hernia
What is a Hiatus Hernia?
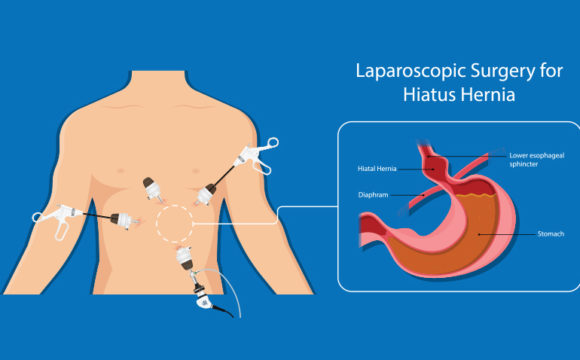
A hiatus hernia occurs when part of the stomach bulges through the diaphragm into the chest cavity through the esophageal hiatus, which is the opening in the diaphragm that allows the esophagus to pass through to the stomach.
Types of Hiatus Hernias
-
Sliding Hiatus Hernia:
- This is the most common type, where the gastroesophageal junction and part of the stomach slide up into the thoracic cavity. It is often asymptomatic but can lead to GERD.
-
Paraesophageal Hiatus Hernia:
- Less common but potentially more serious, this type involves part of the stomach pushing through the diaphragm beside the esophagus, which can lead to complications like strangulation of the stomach.
Symptoms
Many patients with a hiatus hernia may be asymptomatic, but potential symptoms can include:
- Heartburn or gastroesophageal reflux.
- Regurgitation of food or liquid.
- Difficulty swallowing (dysphagia).
- Chest pain or discomfort.
- Belching.
Diagnosis
- Physical Examination: Often includes evaluation of symptoms.
- Imaging Studies: Chest X-ray, barium swallow study, and esophagogastroduodenoscopy (EGD) can be used for confirmation.
Management
- Lifestyle Modifications: Dietary changes (avoiding large meals, spicy or fatty foods), weight loss, and elevating the head during sleep can help relieve symptoms.
- Medications: Proton pump inhibitors (PPIs) and H2 receptor antagonists may be prescribed to manage acid reflux and heartburn.
Surgical Intervention
- Indications for Surgery: Surgery may be considered for symptomatic patients who do not respond to medical management or are experiencing complications (e.g., strangulation in paraesophageal hernias).
- Surgical Techniques: Laparoscopic fundoplication (e.g., Nissen fundoplication) may be performed to correct the hernia and prevent reflux.
Gastroesophageal Reflux Disease (GERD)
Gastroesophageal Reflux Disease (GERD) is a chronic condition where stomach acid flows back into the esophagus, leading to symptoms and complications due to prolonged exposure to gastric contents.
- Lower Esophageal Sphincter (LES) Dysfunction: Inadequate closure of the LES often leads to acid reflux.
- Hiatus Hernia: As previously discussed, can contribute to GERD.
- Obesity: Increased abdominal pressure can exacerbate reflux.
- Pregnancy: Hormonal changes and increased abdominal pressure can affect esophageal function.
- Medications: Certain drugs like NSAIDs, calcium channel blockers, and muscle relaxants can relax the LES.
- Heartburn: A burning sensation in the chest, typically after eating or at night.
- Regurgitation: Return of acidic stomach contents to the throat, resulting in a sour taste.
- Dysphagia: Difficulty swallowing foods or liquids.
- Chronic Cough or Hoarseness: Especially if acid irritates the throat.
- Chest Pain: May be mistaken for cardiac issues.
- Clinical Evaluation: Symptom history and frequency.
- Endoscopy: Esophagogastroduodenoscopy to visualize changes in the esophagus and stomach.
- pH Monitoring: Tests to measure acid levels in the esophagus over 24 hours.
- Manometry: Assessment of swallowing function and LES pressure.
- Lifestyle Modifications: Recommendations include weight loss, dietary adjustments, and elevating the head during sleep.
- Medications: PPIs are commonly prescribed to reduce stomach acid production and protect the esophagus.
- Indications for Surgery: Considered in patients who have severe GERD symptoms that do not respond to medication, or if there are complications such as esophagitis or strictures.
- Surgical Techniques:
- Nissen Fundoplication: A laparoscopic procedure that wraps the top of the stomach around the esophagus to strengthen the LES.
- Toupet Fundoplication: A partial fundoplication that is often used in patients with motility disorders.
Complications of Hiatus Hernia and GERD
- Esophagitis: Inflammation of the esophagus due to persistent acid exposure.
- Esophageal Strictures: Narrowing of the esophagus can occur, leading to swallowing difficulties.
- Barrett’s Esophagus: A precancerous condition resulting from chronic GERD, where changes in the esophageal lining occur.
- Aspiration Pneumonia: In some cases, stomach contents may enter the lungs, particularly in patients with severe reflux not well controlled.
Overview of Fundoplication Surgery
1. Nissen Fundoplication
Definition
Nissen fundoplication is a surgical procedure in which the top portion of the stomach (fundus) is wrapped around the lower esophagus to reinforce the lower esophageal sphincter (LES) and prevent gastroesophageal reflux.
- Gastroesophageal Reflux Disease (GERD): Severe GERD symptoms that do not respond to medical management.
- Hiatal Hernia: Correction of hiatal hernia in conjunction with GERD treatment.
- Esophagitis: Inflammation of the esophagus caused by prolonged acid exposure.
- Barrett’s Esophagus: A precancerous condition resulting from chronic GERD.
- Overview: The procedure can be performed laparoscopically or through an open surgical approach.
- Procedure Steps:
- Anesthesia: The patient is placed under general anesthesia.
- Incision: In laparoscopic surgery, several small incisions are made in the abdomen. In open surgery, a larger incision is made.
- Dissection: The surgeon identifies the lower esophagus and mobilizes the fundus of the stomach.
- Wrap and Fixation:
- The fundus is wrapped around the lower esophagus and secured with sutures.
- The wrap typically encircles the esophagus 360 degrees.
- Closure: The incisions are closed following confirmation of proper placement and function of the wrap.
- Duration: The procedure generally lasts between 2 and 4 hours.
- Hospital Stay: Patients typically remain hospitalized for 1 to 3 days for monitoring.
- Immediate Postoperative Care: Vital signs are monitored, and pain management is provided. Patients are initially restricted to a liquid diet.
- Diet: Gradual reintroduction of solid foods over several weeks as tolerated.
- Common Risks: Infection, bleeding, and complications related to anesthesia.
- Specific Complications:
- Dysphagia: Difficulty swallowing may occur if the wrap is too tight.
- Gas Bloat Syndrome: Inability to expel gas can cause discomfort.
- Recurrence of GERD: Sometimes reflux symptoms may return if the fundoplication is not successful.
- Injury to Surrounding Organs: Risk of damage to the spleen or other nearby structures during dissection.
- Success Rates: Studies indicate a success rate of approximately 80-90% in alleviating GERD symptoms in the long term.
- Quality of Life Improvement: Patients often report significant improvements in quality of life post-surgery, with decreased reliance on medications to control GERD symptoms.
2. Toupet Fundoplication
Definition
Toupet fundoplication is a surgical procedure that involves a partial wrap of the fundus of the stomach around the lower esophagus, typically about 270 degrees, offering an alternative to the complete wrap of Nissen fundoplication.
- Gastroesophageal Reflux Disease (GERD): Indicated for patients who experience severe GERD and may have motility disorders or prior surgical history impacting esophageal function.
- Hiatal Hernia: Correction may be performed alongside the repair of a hiatal hernia.
- Prior Surgery to the Esophagus: Often preferred for patients with risk factors for impaired swallowing, where less tension is applied.
- Overview: The procedure is primarily performed laparoscopically.
- Procedure Steps:
- Anesthesia: The patient is placed under general anesthesia.
- Incision: Laparoscopic techniques involve the creation of several small incisions.
- Dissection: The gastroesophageal junction is mobilized, and the hiatal hernia is repaired if present.
- Wrap and Fixation:
- The fundus of the stomach is wrapped around the esophagus about 270 degrees and then secured with sutures.
- This creates a less restrictive wrap compared to the Nissen procedure but still helps reduce reflux.
- Closure: The incisions are closed following appropriate placement of the fundoplication.
- Duration: The procedure typically lasts about 2 to 3 hours.
- Hospital Stay: Patients usually stay in the hospital for 1 to 3 days, depending on recovery progress.
- Postoperative Care: Frequent monitoring of vital signs and any signs of complications; pain management is initiated.
- Dietary Management: Patients start on clear liquids, gradually progressing to a regular diet as tolerated.
- Common Risks: Similar to those associated with Nissen fundoplication: infection, bleeding, and anesthesia risks.
- Specific Complications:
- Dysphagia: Can occur but is generally less severe than in Nissen fundoplication due to the partial wrap.
- Bloating and Gas: Patients may experience discomfort from gas retention, though typically less than with Nissen fundoplication.
- Recurrence of GERD: While effective, the risk of recurrent symptoms remains.
- Success Rates: Long-term success rates are comparable to those of Nissen fundoplication, generally around 75-85% for the resolution of reflux symptoms.
- Quality of Life: Patients often report satisfactory relief from GERD symptoms and improved quality of life, with less post-operative dysphagia compared to complete wraps.